Health systems frequently ask whether artificial intelligence will ultimately reduce the need for clinicians. Radiology provides one of the clearest real-world answers to date. AI changes the mechanics of work far more than it changes the need for expertise.
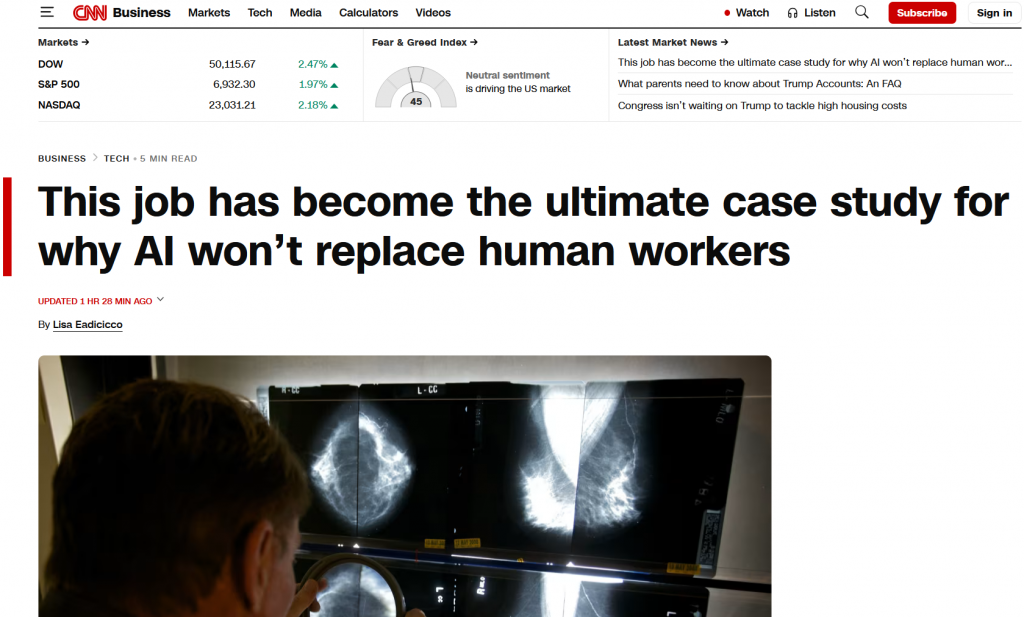
I had the privilege to speak with CNN on this topic recently. The story is out now.
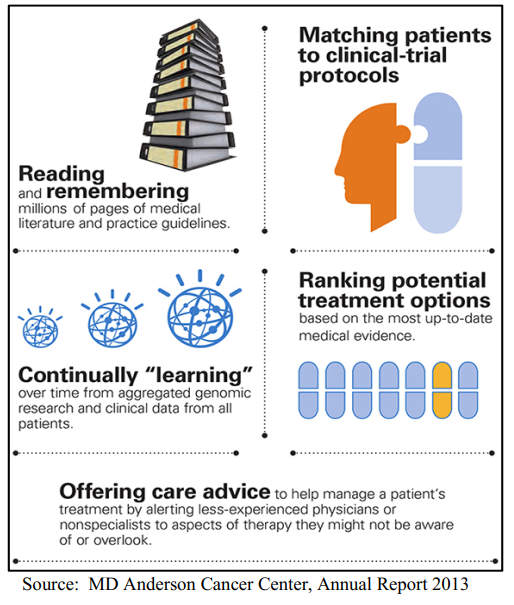
In imaging operations, AI is already being used to support exam prioritization, improve image reconstruction, and reduce friction in routine workflows. These contributions are meaningful, particularly in high-volume environments. But they do not displace clinical judgment, professional accountability, or responsibility for patient outcomes. In practice, the performance gains attributed to AI are inseparable from expert oversight and careful integration into clinical teams.
We use AI as a capacity and quality multiplier, not as a substitute for our training. That line is difficult to walk and gets thinner as products improve, but the thought matters. Deploying it primarily as a justification for workforce reduction or skill substitution introduces avoidable risk to patient safety and physician trust.
Success ultimately go to those investing in workflow, governance structures, and building solution that define clear roles for both humans and machines. Radiology may be an early example, but the underlying lesson extends well beyond imaging.